
Heart and Lung
By Thom Parry
11.09.20
In May 1953, John H. Gibbon, Jr., MD ’27, made medical history by performing open heart surgery with the use of the heart-lung machine, a machine of his own invention. The procedure was the world’s first successful cardiopulmonary bypass surgery. The arc toward this success was not clean. Fatal setbacks occurred. Still, the machine found its purpose and has since saved millions of lives.
Cecelia
Cecelia Bavolek was born with an atrial septal defect, a hole in the muscle wall separating the upper chambers of her heart.
The blood of the chambers mixed, swirling the “blue,” oxygen-depleted blood with the red, oxygen-rich blood. The flow was disordered, and her heart murmured. Over the years, it swelled with pressure and grew too large.
By the time Bavolek was 18 and a freshman at Wilkes College in Wilkes-Barre, Pennsylvania, she was in heart failure. She collapsed again and again. The hole was the size of a silver dollar, the doctors said. If it remained open, she would likely die.
Bavolek and her mother came down to Philadelphia, to Jefferson, in search of help. They met Dr. John H. Gibbon, Jr.
Dr. Gibbon told Bavolek that he had a machine that could, for a while, act as her heart and lungs. It could keep her alive while he closed the hole in her heart.
No human had ever survived this procedure.
Victor Greco, MD ’51, was part of Gibbon’s surgical team.
“I’ll never forget Dr. Gibbon talking to her in a very calm manner, explaining what had to be done,” recalls Dr. Greco.
The heart-lung machine was unknown to the public at large and often decried as a monstrosity and boondoggle among medical doctors. But Bavolek was facing death. She had few options. She agreed to the risk.
The surgery was quickly scheduled for May 6, 1953.
Jack
Decades before, while in his second year at Jefferson Medical College, John H. Gibbon, Jr. told his father that he wanted to quit.
Medicine wasn’t for him, he said. He wanted to write poetry.
The Gibbons were a storied family of Philadelphia’s Society Hill, and John, whom everyone called Jack, was their tall, blue-eyed heir. He was to be the fifth in a line of Doctors Gibbon.
His father, John Gibbon, Sr., MD 1891, a professor and doctor at Jefferson, told Jack to give medical school more time, to see what would come.
Jack obeyed his father, and a few years later, he conceived of a lifesaving machine.
The idea came to Jack late at night while he was sitting at the bedside of a woman who was close to death. She was pale, lethargic. Blood had clotted in the artery between her heart and lung. The embolism had to be removed.
It was 1931, and Jack was then a research fellow at Harvard Medical School. He was keeping a vigil over the patient, monitoring her blood pressure and breathing, waiting for the moment when they could no longer delay the operation. He knew, however, that once they opened her chest, her brain would starve of oxygen and she would die within minutes.
“During that long night, helplessly watching the patient struggle for life as her blood became darker and her veins more distended, the thought naturally occurred to me,” Gibbon later wrote, “the patient’s life might be saved if some of the blue blood in her veins could be continuously withdrawn into an extracorporeal blood circuit, exposed to an atmosphere of oxygen and then returned to the patient…”
The extracorporeal circuit of Jack’s conception would work as the woman’s heart and lungs and keep her brain supplied with oxygen. The machine would allow the surgeon to dilate time, to work in a bloodless field, to see the problem clear and make the repair.
At 8 a.m., time was up. The chief surgeon began the procedure to remove the embolism. The patient died within seven minutes.
-

John H. Gibbon, Jr.
-
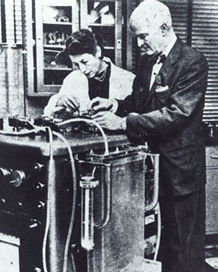
John H. Gibbon, Jr., Mary H. Gibbon, and heart-lung machine, u.d.
The lead technician at that surgery was Mary Hopkinson. Mary, or “Maly” to her friends, had attended Bryn Mawr College, studied piano in Paris, and pursued medical training at Harvard. There, she met Jack. The two married, and together they began work on what would become the heart-lung machine. They spent long days in the lab and talked through their research at night. Within a few years of their marriage, they had published over a dozen papers. Shortly before Jack deployed to the South Pacific as a medical officer during WWII, the couple operated on the heart of a cat. For 10 minutes in the course of that procedure, which was a success, they diverted the feline’s heart and lung function to an early iteration of the heart-lung machine.
In the throes of a joy that Jack would never forget, he and his wife embraced one another and danced around the lab.
History credits John H. Gibbon, Jr. as the inventor of the heart-lung machine, but as Mary Gibbon’s contributions indicate, the machine represented the efforts and intelligence of many. To create the “heart” of the heart-lung machine, the Gibbons used the smooth-running “roller” pumps created by surgeon Michael DeBakey, MD. The lungs were a greater challenge, requiring contributions from several minds. Initially, the Gibbons had trickled blood into a large, rotating cylinder to expose the blood to oxygen, but as they progressed from cats to dogs, they had to increase the surface area, resulting in ever-larger cylinders.
The lungs of an adult human contain 1,500 miles of airways. A heart-lung machine for humans would require spinning barrels a few stories tall.
After WWII, Jack returned to Jefferson to teach, practice medicine, and continue tackling the problems of the machine. At Jefferson, surgical residents and IBM engineers hit upon the idea of running the blood over mesh screens. With this idea, Gibbon and his team managed to recreate the equivalent surface area of a tennis court within a Plexiglas housing the size of a suitcase.
A dozen more problems remained—acidity, blood depletion, pressure, anesthesia, clotting—but solutions arrived as more doctors, students, scientists, and engineers joined the effort. In particular Bernard J. Miller, MD ’43, made crucial contributions working with IBM to improve the device.. By 1952, the team at Jefferson could keep a large dog alive on the machine for an hour and a half. The team would sedate a given dog, cut a hole in its heart with a sharp tube, close the hole, and return the dog to consciousness. The residents kept vigils over them. Dozens of dogs underwent the procedure. Survival rates increased. In early 1953, Gibbon felt it was time to try the machine with a human.
The first patient was a 1-year-old girl. She had been in cardiac failure since birth. When Gibbon opened her chest, he discovered that she had been misdiagnosed. Instead of a hole in the heart’s inner wall as they expected, the girl was suffering from a large patent ductus arteriosus, the failure of a critical blood vessel to close at birth. Her blood was flowing in the wrong direction. She died on the table.
The machine, however, had functioned according to its purpose. Gibbon and his team decided to press on.
-

Seated, Left to Right: Dr. Paul R. Hawley, Dr. E. Gordon MacKenzie, Dr. John H. Gibbon Jr., Dr. John F. Rogers
Standing, Left to Right (IBM Engineers): Robert T. Blakely, G.A.V. Malmros, I. Smith Homans, Jr., J.H. Fraser. -

Dr. Gibbon, Cecelia Bavolek, and the artificial lung.
May 6, 1953
On the morning of Cecelia Bavolek’s operation, Dr. Victor Greco and the other residents wheeled the machine from the “dog lab” on the 10th floor of the College Building to the fourth floor of the “Old Main” hospital next door. The heart-lung machine—a massive, stainless steel box with rows of control dials, knobs, switches, and indicator lights—weighed more than that year’s Volkswagen Beetle.
As Greco recalls, the procedure began with the team administering nerve-blocking shots below Bavolek’s ribs. Throughout her chest, she’d feel nothing. Before she went under sedation, Greco stepped forward and gently sprayed Novocain into Bavolek’s throat as a numbing agent. He then eased a tube into her windpipe to keep the airway open.
Everyone in the operating room was standing in a few inches of water. Gibbon had chosen cyclopropane gas as an anesthetic, a highly reactive gas. The static electricity of a shoe sole scraping the floor could cause an explosion.
Bavolek lost consciousness. Soon after, Gibbon sliced into Bavolek’s chest, cut through her breastbone, and exposed her enlarged heart. He clamped shut the vessels to it and shunted her blood through a tube to the machine.
That May morning was hot and the operating room had no air conditioning. Gibbon had the windows open to the breeze. Outside, however, pile drivers were at work pounding steel beams into the ground for Jefferson’s newest facility, the Foerderer Pavilion. As the concussive thud and ring sounded in the OR, a surgical nurse mopped Gibbon’s brow.
His scalpel had revealed the hole in Bavolek’s heart.
Frank Albritten, MD, an assisting surgeon and key contributor to the team, peered close to document the exposed atrium with a new camera. A flashbulb went off by Gibbon’s neck. Gibbon flinched and swore.
Meanwhile, as intended, oxygen-depleted blood flowed from Bavolek and through a tube that served as her out-of-body artery. Propelled by the mechanical heart of four DeBakey roller pumps, the dark blood climbed to a clear, acrylic tower that housed the aluminum mesh screens. The blood then trickled down over the screens, gathering oxygen and turning bright red.
Everything went as planned, until it didn’t.
At some moment during the 45 minutes in which the machine functioned as Bavolek’s heart and lungs, her blood clotted. The clots first stuck in the mesh of the screens and then traveled down to the bottom of the artificial lung. There, the clots stoppered up the exit tubes. The incoming blood frothed. Bubbles rose.
Greco, who was operating the machine with Gibbon’s head technician, Joan Carruthers, jumped up onto a stool and threw his arms on the lid of the lung’s housing.
“I was afraid the pressure would blow the top of the artificial lung off,” Greco recalls. “You’d have blood all over the operating room.”
“BJ, get over there and do something!” Greco recalls Gibbon saying to Bernard J. Miller, MD, another assisting surgeon.
Dr. Miller, who had made crucial contributions in the machine’s electrical design, dropped out of the surgery, cut the pumps, and operated the machine’s pressure manually.
Gibbon had intended to close the defect with a patch, but time was up. Instead, he sewed the hole closed with a silk thread.
The team removed Bavolek from the machine, and Gibbon watched her heart. It was in spasm, fluttering rather than beating. Gibbon shocked it back into rhythm.
Cecelia and Jack ... Afterward
“I felt it would go my way with Dr. Gibbon’s machine and lots of prayers,” Cecelia Bavolek was quoted in the Philadelphia Evening Bulletin.
“Call it a youthful hunch,” she said. She spent two weeks in recovery and refused to pose for a picture. Dr. Gibbon attempted two more bypass surgeries with the heart-lung machine that year. Both patients were children. Both patients died.
He abandoned the machine and set down his scalpel, never again operating on a heart or performing any surgery.
On request, he shared the machine’s design with the Mayo Clinic in Rochester, Minnesota. The clinic improved the machine, lowering the mortality rate to 10 percent within a few years. The machine has since helped millions of patients survive the peril of open heart surgery.
In early 1960s, as the fame of heart-lung machine was growing, the American Heart Association prevailed upon Bavolek to accept the mantle of the “Heart Fund Queen,” an annual title often bestowed by the likes of Bobby Darin and Bob Hope. And finally, in 1964, Bavolek and Gibbon posed for a picture before the oxygenator. When the camera flashed, Bavolek was looking somewhere beyond that artificial lung. Soon after, Gibbon retired from medicine. On a farm outside the city, he painted and wrote poetry.
In February 1973, a few months prior to the 20th anniversary of the heart-lung machine’s first success, Gibbon collapsed while playing tennis. He died of heart failure.
At his memorial service, friends remembered him as a man who loved to square dance, who would swim in the coldest water, and who never dwelled on the magnitude of his achievement.
Each year, a club called “Gib’s Rib Crackers,” made up of his colleagues and mentees, would celebrate the pioneering doctor. One year, they invited Bavolek as an honored guest. She politely declined, but in seeking her out, the Rib Crackers discovered that Bavolek worked at a hospital in Philadelphia.
Like Mary Gibbons and Joan Carruthers before her, she had become a medical technician. Cecelia Bavolek ran machines to keep people alive, to extend a chance that not long ago, no one would have dared imagine.